Part I is a post on Evidence Based Medicine.
Part II is here.
The SEIU is planning a big push for universal healthcare in this election cycle. The time seems to be here when we have to think about this.
There is a pretty good post over at Megan McArdles blog with the comments as interesting as the post. She links to Paul Krugman, often a source of misinformation. The topic is the Massachusetts Plan that is seeing cost overruns. Every new health care entitlement, from the National Health Service in England to Medicare here, has seen huge increases in cost that were not predicted. There are a number of reasons. One is the moral hazard problem, in which people will sign up for anything that is free.
One of the comments actually poses a nice outline for a solution:
Response to liberalrob’s question “what’s your solution…”:
Sign up everybody who makes above a certain income threshold for some kind of minimal national health plan that covers ONLY catastrophic health costs. Make the cost based on age, and deduct it automatically from their paycheck like Social Security.
Make it voluntary, but auto-opt-in– that is, you’re signed up unless you fill out a form and say “Thanks, but no thanks.”
If you opt-out, decide not to buy insurance, and get sick– tough cookies.
Everybody who makes below a certain income threshold gets automatically signed up for Medicaid, at no cost.
Oh, and of course either get rid of the employer tax deduction for health insurance or extend it so the employees get the same tax break if they buy their own insurance…
Posted by Gavin Andresen
Let’s take these one at a time:
Sign up everybody who makes above a certain income threshold for some kind of minimal national health plan that covers ONLY catastrophic health costs. Make the cost based on age, and deduct it automatically from their paycheck like Social Security.
I am coming to the reluctant conclusion that a single payer plan of some sort is going to be necessary. The German system has two types of insurance, the state system which is deducted from your paycheck, and private insurance, which is available to those with high incomes who choose to opt out of the state system. The original German system had a number of health plans, some employer based and some community-based, but all had to join one unless your income was quite high, at which point you could opt out. The state system deduction is income determined and is about 14% of gross income. The private system is more like American insurance and is risk-determined, by age and state of health. The Clinton Plan in 1994 was supposed to be based on the German system. This is an attractive option for several reasons.
The present American system has a real problem with “free riders.” These are usually young people who are healthy, could afford insurance but choose to go without because they know that, if disaster strikes, they will be cared for and they can evade the cost of emergency care by bankruptcy if necessary. Some years ago, when I was still in practice, the employee of a colleague, a vascular surgeon who had once been in practice with me, contacted my office because she needed gall bladder surgery. She informed my staff that she had no health insurance even though she was employed full-time. I was very annoyed at my colleague for allowing an employee to be uninsured until I learned that she had opted out because she would rather have the extra money as salary. I don’t know that I would have allowed this but, at least, it wasn’t through any greed of his.
There is the classic free-rider. The famous “47 million uninsured” includes millions of these, as many as a third of the uninsured. Federal laws require that doctors and hospitals care for these people in cases of emergency and emergency is pretty broadly defined. The law is quite onerous and carries severe criminal penalties. Therefore, free riders can be assured of care by specialists and hospitals when emergencies require it.
The consequences for everyone else is the removal from the insurance pool of healthy young adults who would be expected to contribute and would have a low level of utilization. The same factors that make them choose free rider status make them attractive for the general pool of subscribers. This is a classic situation of tragedy of the commons. The sheep herder who grazes his sheep in the communal pasture, depletes the resources of the village without contributing his share. He will profit from this free riding until the system collapses, at which point he may make use of the resources he has taken from the common pool and go on his way leaving others to cope with disaster, or he may suffer the same fate, probably blaming ill luck rather than his own anti-social behavior.
This issue raises the question of mandates. Mandates that everyone buy insurance are part of Hillary Clinton’s plan and not Obama’s plan. Krugman says this will make Obama’s plan fail due to the free rider problem and, for once, I agree with Krugman.
There is another group of uninsured and we will deal with them next.
Point two:
Make it voluntary, but auto-opt-in– that is, you’re signed up unless you fill out a form and say “Thanks, but no thanks.”
If you opt-out, decide not to buy insurance, and get sick– tough cookies.
This is attractive emotionally but is a non-starter because of federal laws that will never be repealed. In the old days of 50 years ago, doctors and hospitals could afford to provide a modest amount of free care to the poor because care was mostly not that expensive for the provider. It was time and not material. Now, much of what is provided to the sick and indigent is expensive and the margin of profit to pay for these cases is far smaller than it once was. There has to be a way to eliminate the majority of the uninsured to prevent bankruptcy of the entire system.
A big share of the problem is illegal immigration. A single payer system without barriers to care would be a further incentive for illegal aliens, especially from Mexico, to seek care in the US. There is already a bus service from Tijuana to Los Angeles County Hospital for Mexican mothers of children who are US citizens to obtain US care for these Medicaid-eligible children. Many suspect pregnant women of entering the country to have “anchor babies” in US hospitals. The 14th Amendment guarantees citizenship for all born in the US. This will never be repealed so provision has to be made for the illegals, another large share of the uninsured.
I spend a day a week at LA County Hospital and about 60% of the patients are Spanish speaking, most of those non-citizens who would not join a single payer plan that required contribution from salary. Just as the federal government has to be the only agency that chooses to enforce the border, they are the only agency to pay for the care of those here illegally. Other community services (like schools) are impacted but we are limiting our comments to health care.
What to do with the poor ?
Everybody who makes below a certain income threshold gets automatically signed up for Medicaid, at no cost.
One problem with Medicaid that few understand is where the money goes.
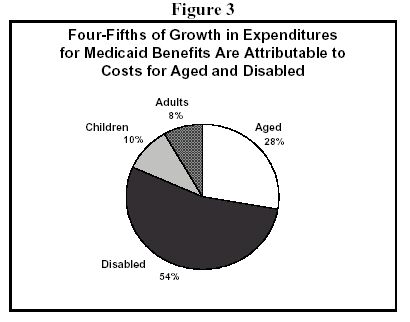
A huge proportion of Medicaid dollars goes to nursing homes and care of the poor elderly. This will rise as the population ages. The rest goes to pregnant women and children with single men being the least likely to participate. Other conditions like mental health and the disabled from other causes round out the rest of the Medicaid population. Medicaid is not just a program for the poor children. What will we do with the nursing home population ? England does much better with home care than we do. Why ? Much of the population of Britain outside of London lives in villages and small cities that lends themselves to residential care. We have more tendency to warehouse elderly poor, perhaps because our population is more mobile and tends to sever ties with the communities we were born in. We may be more likely to end up alone with no family nearby.
Is the present system, such as it is, less expensive than a government program would be ?
That is a big question and will be Part IV.